
What the research does show is that for the right conditions, applied correctly, therapeutic ultrasound reduces pain, improves tissue mobility, and prepares soft tissue for the hands-on work that drives real rehabilitation progress. The key phrase is applied correctly—technique and coupling quality matter more than most practitioners acknowledge.
This article covers what therapeutic ultrasound does, where the evidence supports its use, how misapplication undermines results, and the practical principles that separate effective treatment from wasted sessions.
Key Takeaways
- Therapeutic ultrasound uses high-frequency sound waves for thermal and mechanical tissue effects, distinct from diagnostic imaging.
- Evidence is strongest for myofascial pain and calcific rotator cuff conditions; other applications carry mixed or limited support.
- It works best as preparation for manual therapy or exercise, not as a standalone treatment.
- Continuous transducer movement and proper acoustic coupling are non-negotiable for safe, effective treatment.
- Track outcomes session to session; if progress stalls, adjust the protocol.
What Is Therapeutic Ultrasound?
Therapeutic ultrasound delivers high-frequency sound waves—typically at 1 or 3 MHz—through a handheld transducer and coupling medium into soft tissue, where the acoustic energy triggers biological effects through thermal and mechanical pathways.
Two Delivery Modes, Two Clinical Goals
The frequency and output mode you select determines what happens inside the tissue:
| Mode | Mechanism | Best Used For |
|---|---|---|
| Continuous | Primarily thermal—heats tissue | Chronic conditions, deep tissue relaxation |
| Pulsed | Emphasizes non-thermal effects (acoustic streaming, stable cavitation) | Acute injuries, tissue repair |
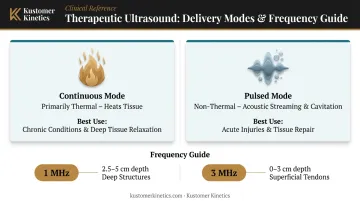
Pulsed mode reduces average energy output but doesn't eliminate heating entirely. A 50% duty cycle can still raise tissue temperature. "Non-thermal" is a relative term here, not an absolute property.
Frequency targeting also matters:
- 1 MHz reaches approximately 2.5–5 cm depth—suited for deeper structures like hip or shoulder musculature
- 3 MHz is absorbed in the 0–3 cm range—better for superficial tendons and ligaments
Therapeutic ultrasound is a preparation and enhancement tool—its job is to make tissue more responsive to the rehabilitation that follows, not to substitute for it.
Key Benefits of Ultrasound in Physical Therapy
Benefit 1: Accelerates Soft Tissue Healing
The proposed mechanism involves fibroblast stimulation: ultrasound-associated increases in intracellular calcium and changes in membrane permeability that support collagen synthesis and tissue remodeling. Stable cavitation (the formation and oscillation of microscopic gas bubbles) and acoustic streaming (enhanced fluid movement at the tissue level) appear to facilitate cellular transport and accelerate repair activity.
These are proposed mechanisms. Animal and preclinical studies have shown meaningful results: one 2016 review found improved collagen alignment and tensile properties in tendon and ligament models, including ligament strength gains around 34%. Those findings don't translate directly to human healing timelines, and clinical interpretation should reflect that gap.
Where the evidence holds up in clinical practice:
- Thermal effects improve local circulation and nutrient delivery to healing tissue
- Non-thermal effects increase cell membrane permeability, supporting repair in tendons, ligaments, and muscle (tendons may heat approximately three times faster than muscle under 3 MHz exposure)
- Calcific rotator cuff tendinitis showed roughly 8.6/100 points greater pain improvement and 14.1/100 greater function improvement at six weeks versus placebo, per a Cochrane review, though evidence quality was rated low
Best applied during: Early-to-mid rehabilitation for acute soft tissue injuries, and chronic cases involving scar tissue adhesions or delayed healing, where stimulating cellular repair activity has direct treatment value.
Benefit 2: Reduces Pain and Localized Inflammation
For patients who arrive guarded, in acute pain, or unable to tolerate manual contact, ultrasound provides a non-invasive way to lower the pain threshold before active therapy begins. Thermal effects relax muscle spasm; mechanical effects may improve local fluid dynamics and reduce inflammatory activity at the cellular level.
The myofascial pain evidence is the most specific and replicable available. In a 54-patient RCT, 10 sessions of continuous 1 MHz ultrasound produced a resting VAS score drop from 5.3 to 1.9, compared to 5.3 to 3.7 with sham treatment, a statistically significant between-group difference (p < 0.001). A 10-RCT meta-analysis confirmed the pain signal (SMD –1.41), though overall risk of bias was rated high.
Practical implications:
- For conditions like myofascial pain syndrome and bursitis, pain reduction often precedes any meaningful active rehab — ultrasound creates that window
- No systemic effects were reported across individual trials, which matters for patients on complex medication regimens or those avoiding injections (though this isn't a direct comparison with NSAIDs or corticosteroids)
When this matters most: Chronic inflammatory conditions, post-surgical soft tissue recovery, and any case where pain is the dominant barrier to functional exercise.
Pain reduction typically registers across several clinical markers: VAS/NRS intensity scores, muscle guarding, starting range of motion at session onset, and patient-reported tolerance during active therapy.
Benefit 3: Prepares Tissue for Rehabilitation
Therapeutic ultrasound earns its place in a multimodal protocol as a setup tool, not a standalone healer. By increasing tissue extensibility and local circulation in a targeted region, it allows manual therapy, stretching, and exercise to be applied to tissue that's already more pliable and better perfused.
One study found that 10 minutes of 3 MHz continuous ultrasound increased active cervical range of motion from 38.5 to 45.4 degrees immediately post-treatment, with effects persisting for approximately 20 minutes, a practical window for follow-on mobilization.
What the evidence does not support: Three sham-controlled trials in frozen shoulder found no consistent added pain or functional benefit when ultrasound accompanied the same exercise and mobilization program. Similarly, ultrasound plus stretching was not superior to stretching alone for knee ligament extensibility in a controlled study.
Ultrasound may improve tissue readiness at the start of a session, but it doesn't appear to produce additive long-term functional gains when layered on already-structured rehab programs — at least not consistently across available trials.
Most useful in these contexts:
- Frozen shoulder (improving initial session tolerance, not replacing mobilization)
- Post-surgical scar tissue management
- Sports injury recovery where progressive loading is the goal
- Chronic contracture conditions requiring repeated tissue preparation
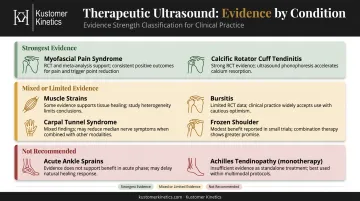
What Conditions Does Ultrasound Treat?
Ultrasound has a well-established clinical history across musculoskeletal conditions — but the evidence quality varies considerably. The table below summarizes where the research stands:
| Condition | Evidence Status |
|---|---|
| Myofascial pain syndrome | Positive pain signal; mixed study results limit certainty |
| Calcific rotator cuff tendinitis | Low-quality positive signal at 6 weeks |
| Achilles tendinopathy | 2024 CPG: do not use as monotherapy |
| Muscle strains | Mechanistic support; limited human clinical evidence |
| Bursitis | Little added benefit shown over exercise + NSAIDs |
| Acute ankle sprains | Cochrane: no clinically important benefit |
| Carpal tunnel syndrome | Insufficient evidence for superiority |
| Frozen shoulder | No consistent added benefit over exercise alone |
Mode selection by condition type:
- Use pulsed mode for acute injuries to deliver mechanical effects without significant tissue heating
- Use continuous mode for chronic conditions to promote deep tissue warming and improve local blood flow
- When in doubt, pulsed mode is the safer default until tissue response is assessed
Key contraindications to know:
- Implanted electronic devices (pacemakers)
- Known or suspected malignancy
- Active bleeding or hemorrhagic disorders
- Pregnancy (over the abdomen/low back)
- Active DVT
- Impaired sensation (requires added caution)
- Treatment directly over the spine or eyes
What Happens When Ultrasound Is Skipped or Misapplied
Skipping ultrasound for a suitable candidate means manual therapy and exercise are applied to unprepared tissue. Patients tolerate less, therapists achieve smaller range-of-motion gains per session, and progress can plateau earlier than expected.
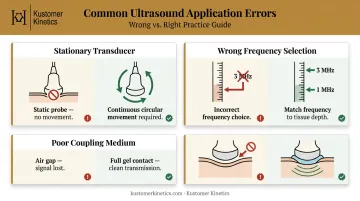
Misapplication produces a different outcome: results poor enough to erode patient confidence in ultrasound altogether. These three errors account for most of those failures:
The three most common errors:
Stationary transducer — Keeping the sound head still concentrates energy in one spot. Clinical guidance requires continuous circular movement throughout treatment. This is a safety and efficacy issue.
Wrong frequency for tissue depth — Using 3 MHz for a deep hip structure deposits energy in the wrong layer. Use 1 MHz for targets at 2.5–5 cm; 3 MHz for superficial structures within 3 cm.
Poor coupling medium — Air between the probe and skin scatters ultrasound waves before they penetrate tissue. Gel and degassed water transmit energy more effectively than mineral oil or petrolatum — and without adequate coupling, the session delivers little therapeutic benefit regardless of other settings.
How to Get the Most Value from Ultrasound in Your Practice
Three Non-Negotiable Application Principles
- Keep the transducer moving in slow, overlapping strokes across the treatment area.
- Match frequency and mode to the tissue: 1 MHz for deeper structures, 3 MHz for superficial targets; continuous mode for chronic conditions, pulsed for acute.
- Follow immediately with rehabilitation. The tissue preparation window is time-limited — passive ultrasound without active follow-on therapy leaves that window unused.
Coupling Quality Is Not Optional
The acoustic coupling medium is what gets ultrasound energy from the transducer into the tissue. Air pockets at the skin surface scatter waves before they penetrate—effectively wasting the session.
Research comparing commercial gels found that tested products transmitted 95–108% relative to degassed water, with differences between products not shown to change patient outcomes. Complete, air-free coupling is what determines transmission quality. A purpose-formulated therapeutic couplant gel—like Kustomer Kinetics' Ultra Gel™—ensures consistent wave transmission and stable transducer contact throughout the session. It's available in bulk formats suited for high-volume clinic use.

Track Outcomes Across Sessions
Treat ultrasound as a clinical tool with measurable impact:
- Record pain scores (VAS/NRS) before and after each session
- Measure range of motion at session start and end
- Document patient-reported function weekly
If scores aren't moving after 3–5 sessions, the protocol needs adjustment—frequency selection, duration, mode, or the condition itself may warrant re-evaluation.
Frequently Asked Questions
What does an ultrasound do in physical therapy?
Therapeutic ultrasound delivers high-frequency sound waves (1–3 MHz) through a handheld probe to penetrate soft tissue, producing thermal and mechanical effects that reduce pain, stimulate tissue repair, and improve circulation. Unlike diagnostic ultrasound, which captures images, therapeutic ultrasound delivers treatment energy directly to tissue.
Can ultrasound break up muscle knots?
Ultrasound can reduce myofascial trigger points by improving local blood flow and tissue extensibility, and the myofascial pain evidence is among the stronger in the field. It works best as a preparatory step before hands-on manual therapy rather than as a standalone treatment for muscle knots.
How much does ultrasound physical therapy cost?
Ultrasound is typically delivered as part of a broader physical therapy session rather than billed separately, so costs vary by clinic, location, and insurance coverage. Out-of-pocket costs depend heavily on your plan and whether you've met your deductible—your clinic or insurer can provide session-specific estimates.
Is therapeutic ultrasound painful?
No—it's non-invasive and generally painless. Patients may notice mild warmth or tingling during treatment. The transducer must stay in continuous motion to prevent discomfort from heat concentration; a properly applied session should feel comfortable throughout.
Who should not receive therapeutic ultrasound?
Individuals with implanted electronic devices (pacemakers), active infections or open wounds, known or suspected malignancy, active bleeding disorders, or pregnancy (treatment over the abdomen) should not receive therapeutic ultrasound without specific physician guidance. Impaired sensation is also a caution flag.
How many ultrasound therapy sessions are typically needed?
Published protocols range widely: 10 sessions for myofascial pain, up to 18 sessions over six weeks for frozen shoulder. There's no universal schedule. Clinicians should track pain scores and range of motion regularly, adjusting the protocol based on measured progress.