Yet despite being widely used across physical therapy clinics, chiropractic offices, and sports recovery facilities, topical analgesics remain poorly understood. Which ingredient works for which condition? When does a cream beat a patch? What separates OTC from prescription strength?
This guide covers all of it: how topical analgesics work, the key active ingredients, OTC versus prescription options, how to match the right product to acute versus chronic pain, and how to use them safely.
Key Takeaways
- Topical analgesics deliver pain relief locally, with systemic exposure up to 6% of an equivalent oral dose
- Topical NSAIDs (diclofenac, ibuprofen) are backed by RCTs and clinical guidelines for acute soft-tissue injuries and knee osteoarthritis
- For neuropathic pain, prescription options—5% lidocaine patches and the 8% capsaicin patch—are the most clinically supported
- OTC counterirritants (menthol, methyl salicylate) offer fast symptomatic relief and remain widely used across physical therapy and chiropractic settings
- Professional-grade formulations are engineered for deeper penetration and consistent dosing—critical for clinical and rehabilitation use
What Are Topical Analgesics and How Do They Work?
Topical analgesics are pain-relieving medications applied directly to the skin—as creams, gels, lotions, ointments, or patches—that act at or near the application site rather than being swallowed and absorbed systemically.
Two Primary Mechanisms
- Peripheral anti-inflammatory action: Ingredients like NSAIDs inhibit cyclooxygenase (COX) activity, cutting prostaglandin signaling and reducing local inflammation at the application site.
- Sensory modulation: Ingredients like menthol or capsaicin alter how peripheral nerve endings perceive and transmit pain signals—independent of any anti-inflammatory effect.
Why Systemic Exposure Matters
FDA labeling for Voltaren Gel (diclofenac sodium 1%) states that normal topical use produces systemic exposure up to 6% of a single oral diclofenac dose. A pharmacokinetic study put numbers to that gap: oral diclofenac produced an AUC0-24 of 3,890 ± 1,710 ng·h/mL versus just 233–807 ng·h/mL for topical regimens.
That distinction is clinically meaningful for patients on multiple medications or with GI and renal conditions—it's one reason topical formulations are often preferred in those populations.
Delivery Formats at a Glance
| Format | Characteristics | Best For |
|---|---|---|
| Gel | Fast-absorbing, water-based | Acute injuries, joints |
| Lotion | Lighter, spreads easily | Larger muscle areas |
| Cream | Water-based, moderate absorption | General musculoskeletal use |
| Ointment | Occlusive, slower release | Dry or thickened skin areas |
| Patch | Sustained, controlled release | Neuropathic pain, prolonged dosing |
One practical limit: topical analgesics work best for pain arising from structures close to the skin—joints, superficial muscles, peripheral nerves. Deep-seated pain from lumbar disc disease or hip joint pathology is generally out of reach. Voltaren Gel labeling specifically notes it has not been evaluated for use on the spine, hip, or shoulder.
Key Active Ingredients in Topical Analgesics
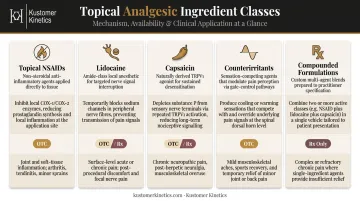
Before diving into individual ingredients, here's a quick reference for how the five main classes compare:
| Ingredient Class | Mechanism | OTC Available? | Primary Use Case |
|---|---|---|---|
| Topical NSAIDs | Inhibit prostaglandin synthesis locally | Yes (diclofenac 1%) | Acute soft-tissue injury, chronic joint pain |
| Lidocaine | Blocks sodium channels in peripheral nerves | Yes (up to 4%) | Neuropathic pain, PHN |
| Capsaicin | Depletes substance P, desensitizes nerve endings | Yes (low %) | Musculoskeletal pain, neuropathy |
| Counterirritants | Activate TRPM8/TRPV1 receptors via competing sensation | Yes | Muscle strains, sprains, joint soreness |
| Compounded formulations | Varies by ingredient combination | No (Rx only) | Complex regional pain, chemotherapy neuropathy |
Topical NSAIDs (Diclofenac, Ibuprofen, Ketoprofen)
These work by inhibiting prostaglandin synthesis locally, reducing both pain and inflammation at the application site without the same systemic load as oral NSAIDs.
The clinical evidence is strong. A systematic review in Mayo Clinic Proceedings found strong evidence for topical diclofenac and ibuprofen in both acute soft-tissue injuries and chronic joint-related pain. Key efficacy benchmarks from a Cochrane overview:
- Diclofenac Emulgel: NNT of 1.8 for ≥50% pain relief at seven days
- Ketoprofen gel: NNT of 2.5 at the same threshold
Voltaren Arthritis Pain Gel (diclofenac sodium 1%) is the main OTC option in the US, available at roughly $19–20 for a 50g tube.
Lidocaine
Lidocaine blocks sodium channels in peripheral nerve fibers, stopping pain signal transmission rather than reducing inflammation.
- OTC ceiling: up to 4% (per FDA OTC Monograph M017)
- Prescription strength: 5% (Lidoderm patch), FDA-labeled for postherpetic neuralgia (PHN)
- A 2009 open-label RCT found the 5% lidocaine plaster had better efficacy than pregabalin in PHN and comparable efficacy in diabetic polyneuropathy
For clinical settings, Kustomer Kinetics' Lido Gel family uses 4% lidocaine in a professional hydrogel format, designed for healthcare practitioner dispensing across physical therapy, chiropractic, and pain management workflows.
Capsaicin
Derived from chili peppers, capsaicin depletes substance P from sensory nerve endings. The initial burning sensation diminishes with repeated use as nerve endings become temporarily desensitized.
- OTC: 0.025%–0.075% creams for minor musculoskeletal pain
- Prescription (Qutenza): 8% topical system, FDA-labeled for PHN and diabetic peripheral neuropathy of the feet
- Must be administered by a healthcare provider
- Treatment duration: 60 minutes (PHN) or 30 minutes (DPN-foot); may not be repeated more often than every three months
Counterirritants (Menthol, Camphor, Methyl Salicylate)
These create a competing cooling, heating, or tingling sensation that overrides pain perception—a process called counterirritation. FDA OTC Monograph M017 defines the approved ranges:
- Menthol: 1.25%–16%
- Camphor: 3%–11%
- Methyl salicylate: 10%–60%
Menthol activates TRPM8 receptors and is widely used in professional formulations for its fast-acting sensory effect and good tolerability. Kustomer Kinetics' Pain Blocker Extra-Strength Analgesic Lotion contains 15% methyl salicylate and 10% menthol—both within FDA-approved ranges—and is used across chiropractic, physical therapy, and sports recovery settings for fast-onset relief from muscle strains, sprains, and joint soreness.
Prescription-Only Compound Formulations
Compounded topicals—ketamine, baclofen, gabapentin, amitriptyline combinations—are used in specific chronic pain scenarios like complex regional pain syndrome or chemotherapy-induced neuropathy. A National Academies review found limited evidence for many of these compounded ingredients and combinations, and they require clinical oversight. They are not standard-of-care options.
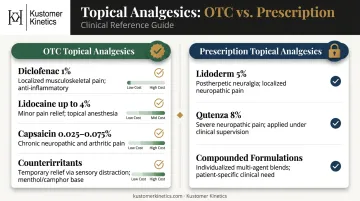
OTC vs. Prescription Topical Analgesics
OTC Options
| Product Type | Examples | Price Range | Best For |
|---|---|---|---|
| Topical NSAID | Voltaren Arthritis Pain Gel 1% | ~$20/50g | Knee OA, hand OA, soft-tissue injuries |
| Lidocaine | 4% creams and patches | $15–25 | Minor pain, localized numbing |
| Capsaicin cream | 0.025%–0.075% | $7–10 | Minor musculoskeletal pain |
| Counterirritants | Icy Hot, Tiger Balm, Pain Blocker | $10–20 | Muscle soreness, acute pain |
OTC options are appropriate for self-management of mild-to-moderate, well-defined musculoskeletal pain. Most clinical guidelines note that sprains and strains resolve within two weeks—if symptoms persist or worsen beyond that point, a healthcare provider evaluation is warranted.
Prescription Options
- Lidoderm 5% patch: For PHN pain; applied to intact skin only
- Qutenza 8% capsaicin: For PHN and diabetic peripheral neuropathy of the feet; clinic-administered only
- Compounded formulations: Ketamine, baclofen, gabapentin combinations for complex cases; limited evidence supports broad use
Professional and Clinical Sourcing
Physical therapists, chiropractors, and sports recovery specialists typically need formulations that go beyond standard retail products—in pack size, clinical performance, and dispensing efficiency. Kustomer Kinetics manufactures professional-grade topical analgesic lines built for exactly these workflows.
Their Pain Blocker lotion line is available in formats from 4oz bottles to gallon sizes with dispensing pumps, supporting both individual treatments and high-volume clinic throughput. Cooling gel options—Polar Relief and Icy Blue Coolant Gel—are formulated for rapid-onset cooling relief in post-adjustment, post-workout, and acute injury applications.
For practices looking to build a branded product line, Kustomer Kinetics also offers private-label contract manufacturing across its full product portfolio, including custom labeling and packaging options. Contact them at 626-445-6161 for wholesale pricing and MOQ information.
Topical Analgesics for Acute Pain vs. Chronic Pain
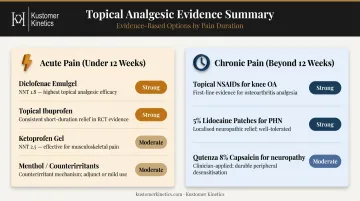
Acute Pain (Under 12 Weeks)
Acute pain—sprains, muscle strains, sports injuries, post-procedure soreness—is where topical analgesics often outperform oral alternatives in clinical practice.
According to an AAFP/ACP guideline summary, topical NSAIDs improve pain within 2 hours, provide sustained relief over 1 week, and are the most effective intervention for improving physical function in acute non-low-back musculoskeletal injuries.
Best options for acute pain:
- Topical diclofenac (Emulgel NNT 1.8 at 7 days) — strongest evidence
- Topical ibuprofen — strong evidence, well-studied
- Topical ketoprofen — well-studied, NNT 2.5
- Menthol/counterirritant products (Pain Blocker, Icy Hot) — fast symptom relief, good tolerability
Cooling gel formats like Polar Relief or Icy Blue are particularly well-suited here—fast onset, non-greasy, and practical in athletic training room and post-adjustment settings.
Chronic Pain (Beyond 12 Weeks)
Chronic musculoskeletal pain—particularly osteoarthritis—and neuropathic pain require a different approach.
For knee osteoarthritis, the 2019 ACR/Arthritis Foundation guideline carries a strong recommendation for topical NSAIDs and explicitly favors local therapy before oral NSAIDs—specifically because topical application limits systemic exposure.
For neuropathic pain (PHN, diabetic neuropathy):
- 5% lidocaine patches — FDA-labeled for PHN; RCT evidence in PHN and diabetic polyneuropathy
- Qutenza 8% capsaicin — FDA-labeled for PHN and DPN-foot; significant pain reduction vs placebo in RCTs
Why this matters for long-term management: FDA labeling for oral NSAIDs states upper-GI ulcers, gross bleeding, or perforation occur in approximately 1% of patients treated for 3–6 months and 2–4% treated for 1 year.
For elderly patients or those with comorbidities, topical analgesics sidestep much of this risk. That safety profile is precisely why ACR guidelines favor local therapy before systemic options.

How to Use Topical Analgesics Safely and Effectively
Correct application technique directly affects both safety and clinical outcome. Here's what practitioners and patients need to know before reaching for a topical analgesic.
Application Best Practices
- Apply only to intact, unbroken skin
- Wash hands before and after (or wear gloves in clinical settings)
- Do not combine with heating pads or occlusive bandages — the FDA warns this can increase absorption unpredictably and risk skin burns
- Avoid contact with eyes, mucous membranes, and open wounds
Dosing Reference (Voltaren Gel, per FDA labeling)
| Joint Location | Per Application | Daily Maximum |
|---|---|---|
| Knee, foot, ankle | 4g | 16g per joint |
| Hand, wrist, elbow | 2g | 8g per joint |
| Total (all joints) | — | 32g/day |
When to Avoid or Seek Medical Guidance
- Salicylate-containing products (methyl salicylate): avoid if allergic to aspirin or taking warfarin—systemic absorption can potentiate anticoagulation
- Topical + oral NSAIDs: Voltaren labeling states this combination has not been evaluated and may increase adverse effects; generally avoid
- Pregnancy: first and third trimesters carry the highest risk; consult a provider before recommending or using any topical NSAID or high-dose salicylate product
- Qutenza (8% capsaicin): never self-apply—requires clinical administration
This guide is informational and does not substitute for professional medical advice. Consult a qualified healthcare provider for diagnosis and treatment decisions.
Frequently Asked Questions
What are topical analgesics?
Topical analgesics are pain-relieving medications applied directly to the skin in forms like creams, gels, patches, or lotions. They work at or near the application site rather than being absorbed systemically through the digestive tract.
What are examples of topical analgesics?
Common examples include diclofenac gel (topical NSAID), 5% lidocaine patches, capsaicin cream, and menthol-based counterirritants like Icy Hot or Tiger Balm. Prescription compounds such as topical ketamine or baclofen are also used for specific chronic pain conditions.
Do topical analgesics really work?
Yes—the clinical evidence is solid for specific formulations. A systematic review in Mayo Clinic Proceedings found strong evidence for topical diclofenac and ibuprofen in acute soft-tissue injuries and osteoarthritis. Lidocaine patches have established evidence for neuropathic pain conditions.
What is the strongest topical analgesic?
It depends on the pain type. For neuropathic pain, the prescription 8% capsaicin patch (Qutenza) delivers the highest available potency. For musculoskeletal and joint pain, prescription NSAID formulations and 5% lidocaine patches are high-efficacy options.
Are topical analgesics safe for long-term use?
Most carry lower systemic risk than oral equivalents because absorption through the skin is substantially reduced. Long-term use should still be monitored by a healthcare provider, particularly for prescription-strength formulations.
Can topical analgesics be used alongside oral pain medications?
Some combinations are acceptable—topical lidocaine alongside acetaminophen, for example. Topical NSAIDs should not be combined with oral NSAIDs, as overlapping mechanisms raise the risk of adverse effects. Consult a provider before combining any treatments.