Topical pain relievers offer a targeted alternative. Applied directly to the skin over the painful area, they concentrate active ingredients at the source without routing everything through the digestive system first. The result: localized relief with fewer systemic side effects than pills.
This article breaks down the four main categories of topical pain relief used for foot pain — counterirritants, topical NSAIDs, capsaicin products, and topical anesthetics — covering how each works, what foot conditions each suits best, and how to choose the right one for your situation.
Key Takeaways
- Topical pain relievers deliver active ingredients through the skin directly to the site of pain — an effective match for foot conditions close to the skin surface
- The four main types work through completely different mechanisms — choosing the wrong one for your pain type means little to no relief
- Match the formulation to the pain type: NSAIDs for inflammatory joint pain, capsaicin for chronic nerve pain, counterirritants for soreness and muscle fatigue
- Topical products carry significantly fewer systemic side effects than oral NSAIDs, but skin safety precautions still apply
- Multimodal formulations combining multiple active ingredients address pain from more than one pathway — useful in clinical settings where single-mechanism products fall short
What Is Topical Pain Relief for Foot Pain?
Topical pain relief refers to any cream, gel, lotion, or patch applied directly to the skin over a painful area. The active ingredient absorbs through the skin rather than entering the bloodstream via digestion, which means faster localized action with less systemic exposure.
The feet are a practical target for this delivery method. Many structures that cause foot pain — joints, tendons, the plantar fascia, and cutaneous nerve endings — sit relatively close to the skin surface. According to StatPearls, the superficial fascia of the foot lies just beneath the skin, and the Achilles tendon is clinically accessible as a superficial structure. That proximity makes topical application well-suited to the feet, unlike deeper joints such as the hip where absorption is far more limited.
Topical pain relievers are available both over the counter and by prescription. Individuals managing chronic conditions use them at home, while physical therapists, massage therapists, and clinical recovery practitioners integrate them into structured care plans. Clinical settings typically rely on professional-grade formulations built for repeated dispensing across multiple patients.
Why Topical Pain Relievers Work Well for Foot Pain
The core advantage of topical application is concentration without systemic exposure. Cochrane research confirms that blood levels after topical NSAID use are typically less than 5% of those achieved after oral dosing — the drug reaches the target tissue without circulating through the entire body.
This specificity matters for several common foot conditions:
- Foot and ankle arthritis — inflammation sits in joints close to the skin surface, making topical delivery genuinely effective
- Plantar fasciitis — the plantar fascia is a superficial structure accessible to topical agents
- Achilles tendinopathy — the tendon is posterior and accessible as a surface-level target
- Diabetic peripheral neuropathy — nerve endings in the feet respond to agents that modulate pain signal transmission

Oral NSAIDs expose the entire body to GI, cardiovascular, and bleeding risks. For superficial foot targets, direct topical application achieves the same or greater localized effect without that systemic burden.
Types of Topical Pain Relief for Foot Pain
Not all topical pain relievers work the same way. Each type uses a different biological mechanism, and matching the right type to your specific pain condition is what determines whether it works.
Some professional formulations combine two or more active ingredient types — called multimodal preparations — to address pain through multiple pathways at once.
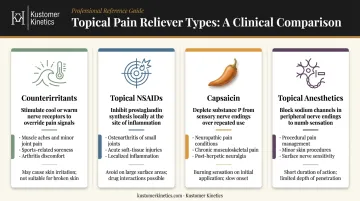
Counterirritants (Menthol, Camphor, Methyl Salicylate)
Counterirritants work by creating a competing sensation — cooling, warming, or tingling — that temporarily overrides pain signals traveling to the brain. The FDA's OTC Monograph M017 defines a counterirritant as a topically applied drug that causes mild skin irritation to relieve pain in muscles or joints.
Menthol activates TRPM8 cold-sensing receptors in sensory neurons; methyl salicylate and camphor desensitize epidermal nociceptors through similar mechanisms.
Best suited for: General muscle soreness, tired or aching feet, mild tendonitis, and post-activity fatigue. They act quickly and can be reapplied as needed.
Formulation note: Gels absorb faster and suit daytime use; creams and rubs linger longer and work well for evening application or massage.
Limitations: Relief is temporary and doesn't reduce underlying inflammation or nerve damage. Not a long-term solution for chronic inflammatory or neuropathic conditions. The strong menthol or camphor scent is a drawback for some clinical settings.
Kustomer Kinetics' Pain Blocker Extra-Strength Analgesic Lotion combines 15% methyl salicylate and 10% menthol in a non-greasy, non-staining formula — a multimodal counterirritant approach used across physical therapy clinics and sports recovery facilities. It's available in sizes up to gallon quantities with dispensing pumps for clinical workflows.
Topical NSAIDs (Diclofenac)
Topical NSAIDs (most commonly diclofenac/Voltaren) absorb into joint tissue and inhibit the same COX enzymes targeted by oral NSAIDs, directly reducing inflammation at the source. A 2020 pharmacokinetic study found diclofenac gel detectable in synovial tissue and fluid 12–15 hours after the last application.
The Voltaren OTC label specifically covers temporary relief of arthritis pain in the foot, ankle, knee, hand, wrist, and elbow — one of the few topicals with explicit foot and ankle labeling.
Best suited for: Foot and ankle osteoarthritis, bursitis, and acute inflammatory flares. A pooled safety analysis found GI adverse events in 25.4% of topical diclofenac users versus 39.0% of oral diclofenac users — a clinically relevant difference for older adults or those with GI sensitivity.
Limitations: Less effective for nerve pain or general muscle soreness. Should not be used simultaneously with oral NSAIDs. Evidence is strongest for superficial joints — foot and ankle arthritis sits squarely within this scope, but plantar fasciitis evidence is limited.
Capsaicin Creams and Gels
Capsaicin (the active compound in hot chili peppers) works by depleting substance P, a neurotransmitter that carries pain signals from peripheral nerves to the brain. With repeated application, TRPV1-expressing nerve endings are desensitized and pain perception decreases over time. Initial applications typically cause a warming or burning sensation that fades with continued use.
Two concentration tiers produce very different outcomes:
- Capsaicin 8% (prescription): An RCT of adults with painful diabetic peripheral neuropathy of the feet found mean pain reduction of -27.4% vs -20.9% for placebo during weeks 2–8. FDA-labeled for diabetic peripheral neuropathy of the feet.
- Low-concentration OTC capsaicin (<1%): Cochrane found insufficient evidence for meaningful benefit over placebo in chronic neuropathic pain, with a number-needed-to-harm of 2.5 for local burning over 6–8 weeks.
Best suited for: Chronic nerve-related foot pain, diabetic peripheral neuropathy, and foot arthritis — when used consistently over weeks.
Limitations: Requires days to weeks of regular application before significant relief. Not suited for acute pain. Hands must be washed thoroughly after application — capsaicin causes significant irritation to eyes and mucous membranes.
Topical Anesthetics (Lidocaine)
Lidocaine works by blocking sodium channels in peripheral nerve endings, temporarily preventing pain signals from being transmitted. When used as directed, only about 3% of the applied dose is absorbed systemically, keeping systemic exposure low.
Evidence for foot-specific lidocaine applications is more limited than for the other types. A Cochrane review found no high-quality RCT evidence supporting topical lidocaine for neuropathic pain, though low-quality data suggest benefit for some patients. Clinical reviews report that 5% lidocaine patches have shown benefit in diabetic neuropathic pain, but the evidence base is smaller and less definitive than for capsaicin 8% in the same indication.
Best suited for: Sharp, localized foot pain with a nerve component — including neuropathy-related sensitivity and post-injury nerve pain. Patches provide sustained relief over several hours without repeated application.
Limitations: Not ideal for broad inflammatory conditions. Patients with severe liver disease or those taking Class I antiarrhythmic medications (such as tocainide or mexiletine) should consult a physician before use.
Kustomer Kinetics' Lido Gel contains 4% lidocaine in a hydrogel format, formulated for clinical practitioner dispensing in physical therapy, chiropractic, and pain management settings.
Quick-Reference: Choosing the Right Type
| Type | Mechanism | Best For | Key Limitation |
|---|---|---|---|
| Counterirritants | Competing sensation (cooling/warming) | Muscle soreness, tired feet, mild tendonitis | Temporary relief only; no anti-inflammatory effect |
| Topical NSAIDs | COX enzyme inhibition | Foot/ankle osteoarthritis, bursitis | Less effective for nerve pain; avoid with oral NSAIDs |
| Capsaicin | Substance P depletion / TRPV1 desensitization | Chronic neuropathy, diabetic foot pain | Weeks of use required; not for acute pain |
| Topical Anesthetics | Sodium channel blockade | Localized nerve pain, post-injury sensitivity | Limited high-quality evidence; not for broad inflammation |
How to Choose the Right Topical for Your Foot Pain
Start by identifying what type of pain you're dealing with — the mechanism determines the match.
| Pain Type | Best-Matched Topical | Notes |
|---|---|---|
| Inflammatory joint pain (swollen, tender joints) | Topical NSAID (diclofenac) | Labeled for foot/ankle arthritis; strongest evidence base |
| Chronic nerve pain / diabetic neuropathy | Capsaicin (8% Rx) or lidocaine | 8% capsaicin has strongest foot-specific RCT data |
| Muscle soreness, tendon fatigue, post-activity ache | Counterirritant (menthol, methyl salicylate) | Fast-acting, use as needed |
| Multifactorial or complex pain | Multimodal/compound preparation | Combines two or more mechanisms |
Formulation type also matters for daily compliance:
- Gels absorb quickly — practical for daytime use or before putting on socks
- Creams and lotions linger longer — better for nighttime or massage integration
- Hydrogel patches provide continuous, hands-free delivery for several hours
Practitioners in physical therapy, sports recovery, and chiropractic settings often need formulations that hold up to high clinical volume. Kustomer Kinetics manufactures Pain Blocker (counterirritant), Polar Relief and Icy Blue cooling analgesic gels, and Lido Gel (topical anesthetic) in bulk and gallon formats with dispensing pumps, and offers private-label manufacturing for clinics that want branded formulations.
For persistent or diagnosed conditions such as osteoarthritis, diabetic neuropathy, or chronic plantar fasciitis, consult a podiatrist or physical therapist. Prescription-strength or compound preparations may be the more appropriate route.
How to Apply Topical Pain Relievers Safely on Your Feet
A few rules apply across all topical types:
- Apply only to intact, unbroken skin — never on open wounds, rashes, or severely cracked skin (common on feet)
- Wash hands thoroughly after application, or wear disposable gloves — especially with capsaicin products
- Do not use with a heating pad or tight bandaging over the application area; heat increases absorption and raises burn risk
- Do not combine topical and oral NSAIDs simultaneously
- If you're allergic to aspirin or take blood thinners, check with your doctor before using products containing methyl salicylate

Individuals with diabetes need to take extra precautions. Reduced skin sensitivity means irritation or burns may go unnoticed until they've worsened. The Qutenza prescribing label requires careful foot examination before each application and use only on dry, intact skin. Consult a podiatrist before selecting any topical for diabetic feet.
Conclusion
Topical pain relievers offer meaningful, targeted relief for foot pain — with a significantly lower systemic risk profile than oral medications. The key is matching the product to the actual cause of pain, not just reaching for the most familiar brand.
Each ingredient class targets a different mechanism:
- Counterirritants address soreness and general muscle fatigue
- Topical NSAIDs act directly on inflammatory joint pain
- Capsaicin — especially at prescription concentrations — has the strongest evidence base for diabetic neuropathy of the feet
- Lidocaine delivers localized nerve-pain numbing with clinically plausible, if limited, evidence
Start by identifying your pain type, then choose the formulation that fits both your condition and daily routine. For chronic, severe, or neuropathic presentations, a podiatrist or physical therapist can guide you toward prescription-strength or compound preparations better matched to your specific situation.
Frequently Asked Questions
Frequently Asked Questions
What is the best topical analgesic for foot pain?
The right choice depends on pain type. Topical diclofenac is the strongest option for inflammatory joint pain in the foot and ankle. Capsaicin (prescription 8%) has the best clinical support for diabetic peripheral neuropathy. Counterirritants like menthol-based gels work well for general soreness and post-activity fatigue.
Is it safe to put lidocaine on feet?
For most people, yes — topical lidocaine is safe for localized nerve pain on the feet when used as directed. Those with severe liver disease or taking Class I antiarrhythmic medications should consult a doctor first. Diabetic patients should exercise extra caution due to reduced skin sensitivity.
Can topical pain relief creams be used for plantar fasciitis?
Counterirritants and topical NSAIDs are the most commonly used options for plantar fasciitis. They can provide temporary pain and inflammation relief, but work best as part of a broader plan that includes stretching and physical therapy — not as standalone treatments.
How often should I apply topical pain relief to my feet?
Frequency varies by product. Counterirritants and topical NSAIDs are typically applied 2–4 times daily as needed. Capsaicin requires consistent multiple-daily applications over weeks before full benefit is felt.
Can I use topical pain relievers on sensitive or diabetic feet?
Use caution. Reduced skin sensitivity in diabetic patients means irritation or chemical burns may go unnoticed. Consult a podiatrist or healthcare provider before selecting a topical, especially for neuropathy-related foot pain, and apply only to clean, dry, intact skin.
Do topical pain relievers for feet have side effects?
Most have minimal systemic side effects compared to oral medications. Local reactions — skin irritation, redness, or burning — are possible, most commonly with capsaicin. Salicylate-containing products carry risks for those allergic to aspirin or on anticoagulants.