Introduction
Most practitioners know ultrasound gel matters. Fewer understand why at the physics level — and that gap leads to poor gel selection, improvised substitutes, and degraded clinical results.
Acoustic impedance is the governing parameter. It determines what fraction of ultrasound wave energy crosses the transducer-skin boundary versus bouncing back unused. When impedance is properly matched, ~99.4% of wave energy transmits into tissue. Introduce even a thin air gap, and that transmission drops to nearly zero.
This guide covers the physics behind acoustic impedance in ultrasound gel, its target value and measurable range, variables that shift it mid-session, and what happens when values fall outside the functional window — for both diagnostic imaging and therapeutic treatment.
Key Takeaways
- Acoustic impedance is defined as Z = ρv (density × speed of sound), measured in MRayl
- Ultrasound gel targets ~1.45–1.5 MRayl to match human soft tissue (~1.6 MRayl)
- Air at 0.0004 MRayl reflects ~99.9% of ultrasound energy — gel bridges that gap
- Temperature, polymer concentration, and drying all shift Z from its rated value during use
- Only purpose-built ultrasound couplants are formulated to meet the soft-tissue impedance target
What Acoustic Impedance Represents in Ultrasound Gel
The Physics of the Parameter
Acoustic impedance (Z) is the product of a medium's density (ρ, in kg/m³) and the speed of sound through it (v, in m/s):
Z = ρv
The unit is the MRayl (megarayleigh = 10⁶ kg/m²s). It quantifies how much resistance a medium presents to acoustic wave propagation, specifically in terms of how the medium responds to pressure oscillations rather than friction.
At any boundary between two media, the ratio of reflected to transmitted energy depends on the difference in acoustic impedance between them. The reflection coefficient (intensity) is:
R = [(Z₂ − Z₁) / (Z₂ + Z₁)]²
A small impedance difference means most energy transmits. A large difference means most energy reflects.
Reference Values That Frame the Problem
| Medium | Acoustic Impedance |
|---|---|
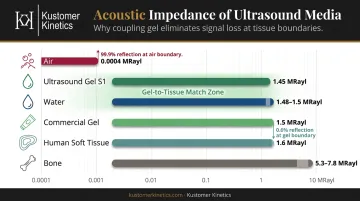
| Air | ~0.0004 MRayl |
| Water | ~1.48–1.5 MRayl |
| Ultrasound gel (S1 formulation) | ~1.45 MRayl |
| Commercial ultrasound gel | ~1.5 MRayl |
| Human soft tissue | ~1.6 MRayl |
| Bone | ~5.3–7.8 MRayl |
Values from Afzal et al. (2022) and Bakhru et al.
The contrast between air and soft tissue explains everything. Air at 0.0004 MRayl versus tissue at 1.6 MRayl produces near-total reflection; lung ultrasound literature reports 99.9% reflection at a soft tissue-air boundary. Gel at ~1.5 MRayl bridges that gap, allowing the vast majority of acoustic energy to transmit into tissue instead.
Why Gel Is a Design Parameter, Not a Byproduct
Ultrasound gel's acoustic impedance is the primary design target, built into the formulation from the ground up. A formulation team developing a couplant is engineering toward the soft-tissue impedance value. Viscosity or optical clarity cannot confirm acoustic suitability on their own.
Factors That Influence Acoustic Impedance in Real-World Operation
Rated impedance values are established under controlled lab conditions — but gel in clinical use is rarely at those conditions. Temperature, formulation concentration, and drying time all shift Z in measurable, predictable ways.
Polymer Concentration and Density
The density component (ρ) of Z is directly affected by how much polymer thickener — typically Carbopol 980 — is present in the formulation.
Research from Afzal et al. (2022) compared formulations ranging from 0.40% to 0.80% Carbopol 980 (w/w). Higher Carbopol concentrations produced higher viscosity, and selected batches yielded impedance values between 1.45 MRayl (low concentration, formulation S1) and 1.5 MRayl (commercial reference gel). Polymer load modulates density, which modulates Z — though the relationship isn't linear or directly proportional to viscosity alone.
Temperature and Speed of Sound
The speed-of-sound component (v) is temperature-sensitive in water-based gels.
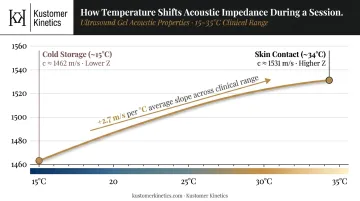
Lubbers and Graaff (1998) derived the water sound velocity formula:
c = 1404.3 + 4.7T − 0.04T² (c in m/s, T in °C)
This yields approximately +2.7 m/s per °C across the 15–35°C clinical range. A gel applied cold from storage and then warmed at skin contact will experience a predictable upward shift in v (and therefore in Z) over the course of a session.
Drying and Gel Ageing
Water evaporation is a genuine coupling risk. A 2024 study on ultrasound coupling gels found conventional gel can lose 22% of its mass (5 g from 22 g) in 15 minutes at 34°C, with air exposure increasing as the gel dries. Polymer density increases as water evaporates, pushing Z upward and eventually creating the air-gap failure case that gel was applied to prevent.
The Target Range for Ultrasound Gel Acoustic Impedance
Nominal Operating Range
The functional target for ultrasound couplant gels is set by the requirement to match human soft tissue (~1.6 MRayl). Peer-reviewed gel formulation research supports 1.45–1.5 MRayl as the validated couplant range, with commercial gels such as Aquasonic 100 measured at ~1.5 MRayl and research formulation S1 at ~1.45 MRayl.
The clinical implication is direct: at a well-matched gel-to-skin boundary, the intensity reflection coefficient is approximately 0.6% — meaning ~99.4% of wave energy transmits into tissue. No formal regulatory standard (AIUM, IEC, WFUMB) has published a numeric acceptable range for couplant impedance; the 1.45–1.5 MRayl figure is research-derived.
Boundary Limits and Tolerance
A practical functional window runs approximately 1.4–1.65 MRayl, under standard conditions: room temperature (~20–25°C), freshly applied gel at full water content, standard polymer concentrations.
| Condition | Z Range | Risk |
|---|---|---|
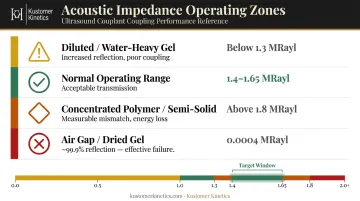
| Diluted / water-heavy gel | Below ~1.3 MRayl | Increased reflection, poor coupling |
| Normal operating range | 1.4–1.65 MRayl | Acceptable transmission |
| Concentrated polymer / semi-solid | Above ~1.8 MRayl | Measurable mismatch, energy loss |
| Air gap (no gel / dried gel) | ~0.0004 MRayl | ~99.9% reflection — effective failure |
Short-session Z drift from temperature or slight drying is generally tolerable. Cumulative degradation across multiple sessions (from water loss, contamination, or improper storage) can push Z outside the functional window with no obvious visual warning.
Why the Margin Matters in Therapeutic Use
The ~0.2 MRayl tolerance on either side of the tissue target is narrower than the numbers suggest. A reflection coefficient rising from 0.6% to several percent compounds across the full beam path — and that loss accumulates at every interface the wave crosses.
In therapeutic ultrasound for physiotherapy or rehabilitation, energy delivery to target tissue is the treatment outcome. Degraded coupling means degraded dose. For diagnostic imaging, the result is reduced image quality; for therapeutic treatment, it is sub-therapeutic dosing at the site that matters.
Key Properties That Shape Acoustic Impedance Performance
Formulation Stability
A well-formulated couplant gel holds its impedance value across its product lifetime. This requires:
- Controlled polymer concentration — Carbopol 980 at defined % w/w keeps density within the target range
- Preserved water-polymer matrix — preservative systems (methylparaben, propylparaben, EDTA as chelating booster) prevent microbial degradation that would otherwise alter density and conductivity
- Accelerated stability testing — Afzal et al. documented viscosity changes of less than 0.1 Pa·s after 7-day accelerated stability testing at 70°C/75% humidity in their optimized formulation, confirming the matrix held
Temperature Sensitivity
Because sound speed rises with temperature in water-based gels, gel used cold from storage and warmed at the skin surface will have a slightly higher in-use Z than its rated value. This is predictable and manageable, provided gel is used within its specified temperature range.
Viscosity as a Contact Layer Tool
Viscosity doesn't determine acoustic impedance — it determines whether the gel stays in place. A gel that runs off the transducer face creates micro air pockets, effectively inserting near-zero impedance zones into the contact layer. This is why adequate viscosity matters: not because high viscosity equals good coupling, but because gap-free contact depends on it. A thick gel with the wrong polymer concentration still transmits poorly — correct formulation and target Z value matter more than viscosity alone.
Kustomer Kinetics' Sonic Scan diagnostic couplant and Ultra Gel therapeutic couplant are purpose-built for clinical couplant applications — distinct from general topicals in the portfolio — manufactured under cGMP-aligned practices in Arcadia, California.
Consequences of Acoustic Impedance Outside the Target Range
When gel Z deviates from soft-tissue matching, the reflection coefficient at the gel-skin boundary rises. The numbers tell the story clearly:
- Gel at 1.5 MRayl vs. soft tissue at 1.6 MRayl: ~0.6% reflection, ~99.4% transmission
- Air vs. soft tissue: ~99.9% reflection, near-zero transmission
The practical failure modes include:
- Diagnostic imaging: Reduced signal strength returns blurred or low-contrast images; depth penetration suffers as compounded reflection losses reduce returning echo amplitude
- Therapeutic ultrasound: Target tissue receives a sub-therapeutic energy dose; in physiotherapy and rehabilitation, this directly undermines treatment efficacy — not just image quality
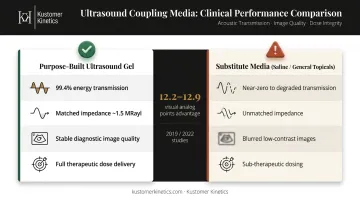
- Substitute media: Gel outscored saline by 12.2 points in a 2019 vascular imaging study and by 12.9 visual analog points (60.9 vs. 48.0) in a 2022 regional anesthesia study — saline and general topicals are not engineered to match the 1.5 MRayl target
These performance gaps have compliance implications. AIUM guidance addresses couplant safety and infection control protocols but does not specify a numeric impedance acceptance range. Even so, using non-validated substitutes in regulated clinical settings exposes practitioners to liability and conflicts with established standards of care.
Common Misinterpretations of Acoustic Impedance in Practice
Three errors come up repeatedly among practitioners:
1. Assuming any clear gel will work Not every water-based, viscous gel qualifies as a medical ultrasound couplant. KY jelly, moisturizing cream, aloe gel, and saline all have different density-speed profiles and have not been engineered to the ~1.5 MRayl target. Choosing a couplant specifically formulated as an acoustic couplant — such as Kustomer Kinetics' Sonic Scan or Ultra Gel — removes this variable entirely.
2. Treating viscosity as a proxy for impedance A thick gel feels substantial and stays on the skin — but that says nothing about acoustic coupling quality. Viscosity and impedance are separate properties. Polymer concentration governs density and therefore Z. A highly viscous gel with the wrong formulation can transmit poorly while appearing clinically appropriate.
3. Ignoring temperature effects A gel rated at room temperature does not necessarily perform the same when applied to a patient with elevated skin temperature — or when drawn from refrigerated storage. Temperature shifts measurably affect Z. Use gel within its specified temperature range to maintain rated performance.
Conclusion
Acoustic impedance isn't a secondary spec on a product datasheet — it's the number that determines how much of your transducer's energy actually reaches the patient's tissue. Gel composition, viscosity, and packaging all matter, but none of it counts if the impedance mismatch at the skin interface is scattering energy before it travels an inch.
Published rated values give you a baseline. Knowing what shifts Z under real conditions — temperature, polymer concentration, water evaporation, gel age — and where the functional window sits means your coupling performance holds up through a full clinical day, not just the first scan.
Frequently Asked Questions
What is the acoustic impedance of ultrasound gel?
Medical-grade ultrasound gel is formulated to achieve an acoustic impedance of approximately 1.45–1.5 MRayl, close to the soft-tissue reference value of ~1.6 MRayl. This value is governed by the formula Z = ρv, where ρ is gel density and v is the speed of sound through it.
Why is acoustic gel used in ultrasound imaging?
Air between the transducer and skin has an acoustic impedance of ~0.0004 MRayl — an extreme mismatch with soft tissue that causes ~99.9% reflection of ultrasound energy. Properly formulated gel closes that gap, allowing ~99.4% of wave energy to transmit into the body.
What happens if no gel is used during an ultrasound?
Without a couplant, air trapped between transducer and skin reflects virtually all ultrasound energy back to the transducer. In diagnostic imaging this produces a severely degraded or unreadable image; in therapeutic ultrasound it means near-zero energy delivery to target tissue.
How does temperature affect the acoustic impedance of ultrasound gel?
Speed of sound increases with temperature in water-based gels (approximately +2.7 m/s per °C across the clinical range), causing a measurable upward shift in Z as gel warms during use. Keep gel within its specified temperature range to ensure consistent acoustic performance throughout the procedure.
Is acoustic impedance the same across all ultrasound gel formulations?
No. Acoustic impedance varies with polymer concentration, water content, and formulation composition. Only gels engineered to match soft-tissue impedance (~1.5 MRayl) are appropriate as ultrasound couplants — general topicals and lubricating jellies are not suitable substitutes.
Can you use ultrasound gel for radio frequency procedures?
Ultrasound gel is not designed for RF (radio frequency) procedures. RF applications require electrically conductive media rather than acoustic couplants. Use a conductive gel or cream formulated specifically for RF to ensure proper current delivery and patient safety.